
















Decolonisation and Global Health
https://doi.org/10.71609/iheid-bd1q-jp90What does it mean to decolonise global health? This question demands an urgent answer as global health is currently in a crisis, due in part to the COVID-19 pandemic, but also to structural factors that produced and defined global health as a field of practice in the first place. Nowhere is this crisis more apparent than in the ongoing descent into a “vaccine apartheid”[1] revealing the failure of the “beautiful idea”[2] of international solidarity.
COVID-19 turned global health into haute politique on par with conflict, terrorism and trade. The pandemic’s devastating effects on lives, health and the economy as well as the frequently ensuing social and political polarisation have become key to domestic and international agendas. The diplomats, philanthropists and academics who make up much of the Global Health system are buzzing with the preparation for the Special Session of the World Health Assembly, considering the necessity of setting up a new pandemic treaty.[3]
Global health policies and resource allocations are determined by global health governance and finance institutions located in the Global North and rooted in colonial practices and epistemologies. But while there are growing calls to decolonise global health, there has been little clarity as to what this would look like in practice.
The Asymmetrical Nature of Global Health

Global health, which started in service of colonial empires with programmes such as the elimination of yellow fever in Panama and hookworm in the Philippines in the first half of the twentieth century,[4] continues to employ many of the same epistemologies and methods that have plagued it from its inception. This is seen in vertical disease programmes that ignore local health and socioeconomic factors and in the emphasis on technical expertise from the Global North over local knowledge and experience. No wonder the map of winners and losers of the COVID-19 vaccination race is almost indistinguishable from that of European colonialism and colonies of a century ago.
In a truly colonialist fashion, the current global health regime seems to carry its “healing mission” despite the people rather than with and for them. It appears to be pursuing two diametrically opposed objectives:[5] protecting the rich from emerging diseases while nurturing a humanitarian biomedicine regime that treats the diseases of the poor. In a truly colonialist fashion, the current global health regime seems to carry its “healing mission” despite the people rather than with and for them. The first objective, however, ordinarily takes precedence over the second as global health governance functions within the limits of state sovereignty[6] and a dominant neoliberal “deep core”[7] that determines its potentialities, priorities and financing. Such a framework is limiting and often subordinates people’s health to the foreign policy and financial interests of powerful states and corporations.
By the same token, the current global health regime tends to generalise technical solutions from high-income settings, applying them to the Global South unadjusted to local context, logistical feasibility and funding limitations. This translates into Western-style healthcare stripped down to barebones and planted in a low-resource setting with little consideration for effectiveness, existing structures, local health-seeking behaviour or sustainability. Another detrimental effect of the prevalence of such isomorphic mimicry is that failure remains accepted as long as the appearance of continued functioning is ensured.[8]
Finally, every global health crisis, from cholera in Haiti to Ebola in West Africa to the current pandemic, is seen and addressed as a separate phenomenon where weak health systems are only the result of current corruption rather than colonial legacies. Such dehistoricisation of global health and its colonial origins[9] serves an implicit ideological function of “legitimising and reproducing the existing power structure in addition to its explicit goal of improving population health and health equity”.[10]
The Coloniality of Global Health

Objections to decolonising the global health regime have emphasised that it might cause resistance to change rather than encourage reforms. It has been argued, for instance, that it could hamper the actual decolonising goal of the repatriation of indigenous people and the return of their land in remaining settler colonialist societies such as the United States, Canada, Australia and New Zealand.[11]
To further the argument beyond the ideological and simplistic, we will employ the notion of coloniality as conceived by Anibal Quijano: unlike colonialism, coloniality “refers to long-standing patterns of power that emerged as a result of colonialism, but that define culture, labour, intersubjective relations, and knowledge production well beyond the strict limits of colonial administrations”.[12]
The coloniality of global health is commonly understood as an expression of the domination of ex-colonial nations over health policy and practice. It imposes a Western understanding of health and disease – inherent in its universalising morality – at the expense of alternative approaches and worldviews. The coloniality of global health translates in its every aspect: its governance structures concentrate in the Global North, producing and distributing knowledge that reflects Western epistemic bias and an implicit distrust toward the people it is supposed to serve. It perpetuates health methods and policies developed by and for colonial administrations.[13]
While arguments about the coloniality of global health knowledge and practice and the need to decolonise are plenty[14], much less, however, is available on the process and actions required to achieve that aim.
How to Decolonise Global Health?
A decolonial discourse on global health rejects the concentration of such necropolitics of global health[15] where a small outsider elite gets to determine what health interventions get implemented in what context, what resources go to whom, and, in short, who lives and who dies. It asserts that true progress towards health equity cannot happen without its decolonisation.[16] Like with the struggle for national liberation, there is no one-size-fits-all approach to decolonising global health. Suggestions have so far wavered between the possibility of reforming the global health regime through quantifiable, if yet unproven, steps to “decolonise” global health organisations”[17] and the radically opposed alternative of upending the system through a Fanonian moment of departure[18] articulating “a new language and a new humanity” and replacing the existing powers with new ones.[19]

Ultimately, there might not be a definitive recipe for decolonising global health. However, fragments of what would be necessary can still be discerned.
First, moving global health governance from a secretive high-diplomacy affair into the public arena. Decolonisation cannot happen without democratisation and the inclusion of the voices of those people most affected by global health issues. This will happen through emancipating global health governance from the domination of a small elite of mostly white Western men[20] by adopting more diverse governance models. It is also necessary to go beyond the narrow and often counterproductive “diversity and inclusion” peformativity[21] by giving greater autonomy of decision over health interventions and their implementation to the communities who suffer ill-health or are at disproportionately high risk of it.
It is also imperative to adopt more transversal approaches coupling global health issues closely to other social justice issues such as climate justice, racial justice or epistemic justice. The consequences of these inextricably linked issues frequently affect the same people. The climate crisis will widen infectious disease endemicity and increase hunger. Forced displacement and race have become determinants of health even in rich societies. None of those issues can be addressed in isolation.
Finally, we cannot but realise that decolonising global health governance is at the heart of all decolonial efforts at emancipation as no real progress towards development or justice for people and communities suffering poverty, discrimination, gender oppression and other forms of supremacy can be achieved while they are suffering the constant risk of ill-health.
Electronic reference
Kirpalani, Dena Arjan, Sara L.M. Davis, and Tammam Aloudat. “Decolonisation and Global Health.” Global Challenges, no. 10, October 2021. URL: https://globalchallenges.ch/issue/10/decolonisation-and-global-health. DOI: https://doi.org/10.71609/iheid-bd1q-jp90.This issue has been produced by the Department of International History and Politics in collaboration with the Geneva Graduate Institute’ Research Office. It also includes contributions from other research centres and departments of the Institute.
Three Maps on Decolonisation
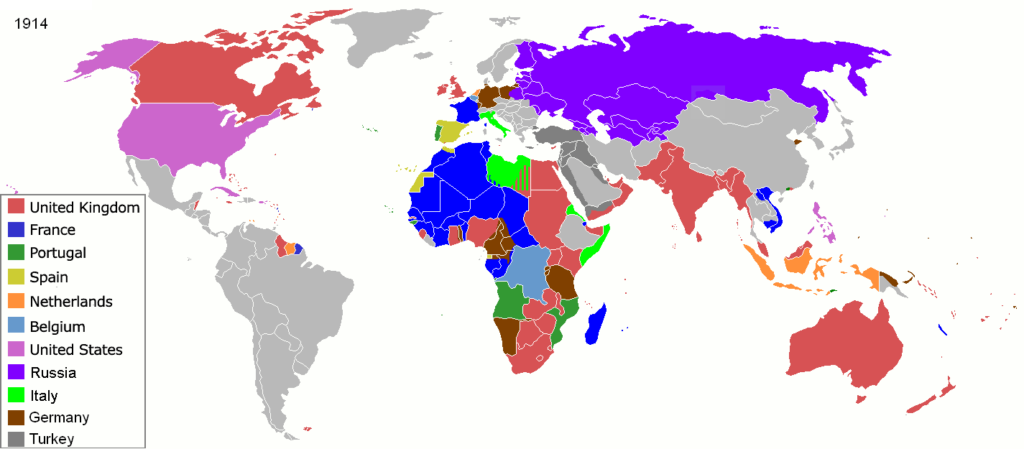


Wikipedia; United Nations
Video | Decolonising Knowledge: A Historical Perspective from Socio-Anthropology – Prof. Shalini Randeria interviewed by Prof. Grégoire Mallard
The Graduate Institute, Geneva
Video | A Brief History of Decolonisation by Prof. Mohamedou
The Graduate Institute, Geneva
Podcast | Décolonisation et impacts institutionnels en Afrique, par le prof. Eric Degila
Graduate Institute, Geneva
Podcast | Le colonialisme vert, par le prof. Marc Hufty
Research Office, The Graduate Institute, Geneva
Podcast | Decolonising the University Space, by Gaya Raddadi
Research Office, The Graduate Institute, Geneva
Podcast | Decolonisation and International Organisations, by Prof. Julie Billaud
Research Office, The Graduate Institute, Geneva
Podcast | Peuples autochtones et décolonisation en 2021, par la prof. Isabelle Schulte-Tenckhoff
Research Office, The Graduate Institute, Geneva
Podcast | Decolonising the Psyche, Prof Mischa Suter
Research Office, Graduate Institute, Geneva
Box | Les empires secondaires de Sa Majesté la reine d’Angleterre
Le Raj victorien, instauré sur les décombres de la compagnie à charte de l’East India Company, a pris la forme d’une vice-royauté qui ne dépendait pas du Colonial Office à Londres et administrait la souveraineté britannique en Asie du Sud et du Sud-Est à partir de New Delhi. Dans l’entre-deux guerres, la moitié des fonctionnaires du Civil Service étaient Indiens. Mais, dès les années 1920, la Grande-Bretagne renonça à l’idée d’une citoyenneté impériale digne de ce nom dont les Indiens eussent été les grands bénéficiaires, forts de leur prééminence non seulement en Asie du Sud et du Sud-Est mais aussi en Afrique australe et orientale, ainsi que dans le golfe Persique. Soucieuse de «britannifier» l’Empire, craignant la montée du nationalisme hindou, soumise à la pression des White Settlers, s’employant à coopter des auxiliaires autochtones, ayant renoncé au «travail contractuel» (indentured labor) qui avait envoyé des sujets du sous-continent indien en Afrique, dans le Pacifique et dans les Caraïbes, se refusant à ériger le Raj en dominion alors que les White Dominions connaissaient une ascension impressionnante, l’Angleterre, qui avait déjà renoncé à instaurer la domination de ce dernier sur la Mésopotamie et le Tanganyika, déçut définitivement ses espérances coloniales et les rabattit sur la revendication de l’indépendance qu’incarnera Gandhi, assez tardivement converti au nationalisme.
L’Égypte, de 1882 à 1914, fournit un autre cas d’empire-gigogne. Investi par le sultan ottoman, son pacha – souverain de fait, héréditaire depuis 1841, et pourvu du titre de khédive à partir de 1867 – fut soumis à la suzeraineté du Royaume-Uni à partir de 1882 et partagea alors avec celui-ci la domination coloniale du Soudan, conquis dès 1820. De la sorte, le Soudan est bel et bien une postcolonie, si l’on accepte le terme, et ce à double titre: par rapport à Londres, et par rapport au Caire. Son histoire contemporaine a démontré que le «néocolonialisme» égyptien était aussi virulent que le britannique, si l’on en juge par ses ingérences dans les affaires de Khartoum. Par ailleurs, la conscience nationaliste égyptienne, antibritannique, fut compatible avec des sentiments de loyauté à l’égard du sultan, ou peut-être plutôt du calife ottoman, jusqu’à la fin de la Première Guerre mondiale.
Le cas le plus intéressant de ces constructions impériales baroques est peut-être celui de l’Afrique du Sud, du fait de l’antagonisme entre les Boers et les Anglais et de l’apartheid qu’institua son architecture composite. La domination britannique se superposa à la colonie hollandaise du Cap et entraîna l’exode d’une partie des Afrikaners à l’intérieur des terres en provoquant in fine le combat fratricide – du point de vue de l’impérialisme européen – entre les deux éléments principaux de la Whiteness. L’objectif de la Grande-Bretagne était de garder le contrôle d’une région dont le potentiel économique et les ressources minières ou agricoles paraissaient énormes, et d’éviter en conséquence la constitution d’États-Unis d’Afrique du Sud qu’auraient dominés les Afrikaners. En 1910, il en résulta l’Union d’Afrique du Sud (Union of South Africa, en français Union sud-africaine) : un régime national de ségrégation raciale dans une économie capitaliste à la fois protectionniste et intégrée au marché mondial, que finit par gouverner et définir l’élite politique des Boers vaincus militairement, par le biais du régime parlementaire, et doté d’un statut de dominion de Sa Majesté (jusqu’en 1961). Mais l’histoire ne s’arrêta pas là. Outre la surexploitation, la dépossession et la relégation raciale qu’elle imposa aux peuples indigènes, elle se traduisit par un afflux de ressortissants du sous-continent indien – les Bataves avaient déjà importé des esclaves malais au Cap –, de réfugiés ou d’immigrants économiques d’Europe orientale, centrale et méridionale qui voulurent profiter du boom minier et firent de l’Afrique du Sud un tremplin pour pénétrer l’Afrique australe et centrale, de Portugais soucieux de s’enrichir mais aussi de fuir les incertitudes de l’accession du Mozambique voisin à l’indépendance. Dans le même temps, l’Afrique du Sud était devenue elle-même une puissance coloniale en ayant obtenu le mandat de la Société des nations, puis la tutelle des Nations unies sur le territoire allemand du Sud-Ouest africain (l’actuelle Namibie), et un hégémon régional en intervenant plus ou moins ouvertement dans les pays voisins, en particulier en envahissant l’Angola pour lutter contre le MPLA aux côtés de l’UNITA dans la foulée de la décolonisation portugaise. L’autre face de la combinatoire impériale fut celle des forces anticoloniales. Non sans éviter leurs propres inimitiés complémentaires qui néanmoins n’égalèrent jamais les contradictions fratricides du mouvement communiste en Indochine, le MPLA, la SWAPO et l’ANC – les trois principaux mouvements de libération nationale en Afrique australe – firent plus ou moins front commun contre leurs adversaires locaux et contre l’apartheid sud-africain et rhodésien en bénéficiant du soutien diplomatique ou militaire, parfois ambigu, des «pays frères», la Zambie, la Tanzanie, le Mozambique (à partir de 1975) et le Zimbabwe (à partir de 1980).
Il va de soi que la problématique de la décolonisation n’a pas été la même d’un «empire secondaire» à l’autre.
Jean-François Bayart.